Shock Types Symptoms Diagnosed Management
Definition of Shock:
The term ‘shock’ means a condition in which essential activities of the body are greatly depressed, especially the volume of circulating blood. The vessels become dilated and do not respond to nervous stimuli. Shock may be caused by pronounced loss of blood. Shock may occur during times of stress, strong emotion, injury, pain, sudden illness and accident. If a state of shock continues over a period of only a few hours, it may be fatal or cause permanent damage to essential organs such as the brain.
Measures which alleviate the shock state are equally useful in preventing it in situations where shock is to be anticipated.

Why do shocks happen:
Shock may begin with a sudden or gradual feeling of unusual weakness or faintness. There be an accompanying pallor. Perspiration is increased and the skin may feel cold and clammy. The pupils of the eyes become noticeably enlarged.
Shock is also accompanied by changes in the mental state and in the pulse beat. The shock patient’s mental attitude follows a pattern, ranging from a feeling of restlessness in the beginning to a gradual loss of ability to respond to stimulation, and finally stupor and unconsciousness. The pulse may seem weak or almost imperceptible; yet it may retain a regular rhythm.
However, when shock is accompanied by (or caused by) loss of body fluids, as in hemorrhage or in cases of severe burns, the pulse rate usually is rapid. Shock is accompanied by myocardial depression and a depletion of the compound ATP (adenosine triphosphate) that aids heart contraction. The physician counteracts this by administering ATP to restock the depleted store and to stimulate heart action.
Symptoms of Shock:
The symptoms of shock are caused to a significant degree by the decrease of the volume of blood in effective circulation and to a lowering of blood pressure. Decreased blood supply to the brain causes mental apathy and may eventually lead to unconsciousness. Lack of blood in the capillaries near the surface of the body accounts in part for the coldness of the skin; evaporation of unusual amounts of perspiration also contributes to the lower body temperature.
When the heart is only partly filled by the smaller amounts of blood, the beat will be noticeably weaker since less blood is ejected at each contraction. When the volume of blood becomes too small, as with the loss of one to two pints through rapid hemorrhage, the heart will compensate to some extent by beating more rapidly. Breathing may become rapid and shallow because the brain is not being supplied with sufficient oxygen.
Shock Diagnosed and Management:
The physician is able to deal effectively with shock by administering blood or blood substitutes to increase the circulating fluid volume, and by treatment for the original cause. This original cause may be nervous in nature, stemming from the effects upon the circulatory system of a psychic reaction to pain and other factors: it may stem from the actual wounding, through accident or surgery, and may not appear for two or four hours after the injury: it may also, as mentioned before, be caused directly by loss of body fluids.
Shock Management:
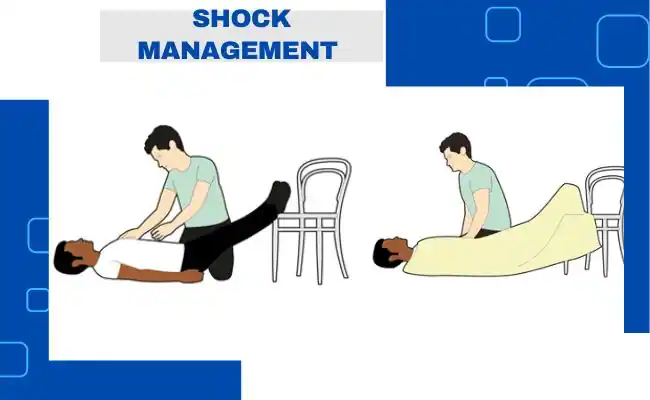
The shock victim should be made as comfortable as possible in a recumbent position. The head should be kept level. A pillow should not be used. It is better if the hips and feet can be raised higher than the head in order to facilitate the passage of blood to the brain.
The patient should be covered with clothing or blankets to maintain body warmth. In cold, equal care should be taken to see that he is protected from the cold ground. This can be done by placing newspaper or blankets beneath the patient or between the springs and mattress of his bed. However, it is undesirable for the patient to become too warm.
Any constricting clothing, such as a collar or belt, should be loosened to avoid interference with respiration or circulation. Stimulus, such as hot coffee or tea without milk or cream, may prove helpful. However, if the patient is unconscious, no fluids should be given, since they may enter the lungs and cause harm. One or two aspirin tablets may be administered to a conscious patient to alleviate pain.
If shock occurs from burns, large amounts of fluid are lost from the tissues. These fluids are salty and must be replaced at once. Treatment for shock consists partially of infusing blood or plasma into the patient’s vein. This must be done by a doctor, a nurse, or some other specially trained professional. However, persons in shock can be given first aid. If the patient is conscious, have him drink a salt-soda solution slowly, and nothing else. If nausea or vomiting occurs, stop giving the solution.
Types of Shock and Treatment:
1. Diabetic Shock:
In diabetic shock the patient breathes deeply and rapidly, and his skin is cold and dry. The breath usually has an odor of acetone. In some cases this has been erroneously ascribed to alcohol and the patient is treated for intoxication. Diabetics usually carry on their persons a card with instructions as to what to do in case of shock. There is no effective first aid treatment (except artificial respiration if breathing has ceased) other than following directions on such a card and calling a physician.
2. Insulin Shock:
Diabetics are also subject to insulin shock, brought on by an overdose of insulin, by failure to eat enough food to neutralize the insulin, or by the accidental injection of insulin directly into a vein. If a person in shock can be questioned and it is found that he has failed to eat for several hours after a dose of insulin, he should be given an immediate source of sugar, such as a candy bar, any bottled or canned soft drink, or sugar itself. Caution must be used, however, since if the patient is actually in diabetic shock (failure to have sufficient insulin) instead of insulin shock (having an excess of insulin), his condition can be aggravated.
3. Electric Shock:
A person suffering from electric shock must first of all be removed from contact with the current. The first-aider must use extreme caution in this procedure. He should not touch the victim directly, nor by means of a metal or wet object. Dry rope, a wooden stick (such as a broom), or a leather belt thrown to stop the current, or the wire may be cut. In cutting the wire, one should use some cutting object with a dry wooden handle, such as an ax.
He should protect his own face and person from the sparks which will fly when the wire is cut, and from contact with the live cut end of the wire. Clothing about the neck should be loosened to facilitate breathing. The patient must be given mouth-to-mouth resuscitation if he is not breathing. The victim is likely to be stiff because of the volume of electricity. Internal injuries and fractures may have occurred.
If the current passed through the central nervous system, the respiratory center of the brain may have been affected. If so, the patient will have ceased breathing. Artificial respiration should be begun at once and continued until the patient begins to breathe. This may take hours: hence, it is desirable to summon the fire Department, or a First Aid Corps that has a resuscitation unit.
In Case of Shock, What You Should Do:
- Do put the patient on his back if he is unconscious. If there is head injury, keep the patient level. Keep the body warm, underneath as well as on top. If cold, apply external heat by use of hot water bottles, if possible, but be careful not to burn the patient.
- Do, if the patient is conscious, place him on his back or stomach, with his head turned gently to one side.
- Do keep air passages open. Clothing about the neck should be loosened to facilitate breathing. Mouth-to-mouth resuscitation must be given if the patient is not breathing.
- Do raise the patient’s hips and feet above the level of his head.
- Do give the patient salt-soda solution to drink in shock following burns if the patient is conscious.
In Case of Shock, What You Should not Do:
- Do not move the patient unless it is absolutely necessary.
- Do not have the patient sit up except in the event of chest injuries or nosebleed.
- Do not use a pillow under the head.
- Do not give a stimulant if there is severe bleeding, either extremely or internally, or if the patient is suspected of having a fractured skull, or has a strong, rapid pulse and red face, as in sunstroke.
- Do not attempt to make an unconscious person drink anything.
- Do not overheat the patient by excess covering.